Shield Report 2011 |

|
VC Moore, AS Robertson, EE McGrath and PS Burge. Occupational Lung Disease Unit, Heartlands Hospital, Bordesley Green East, Birmingham B9 5SS
SHIELD is the Midland Thoracic Society’s Surveillance Scheme for Occupational Asthma for the West Midlands. The scheme, which was set up in January 1989, was established to study the general and specific incidence of occupational asthma within the West Midlands region and Metropolitan County. The rate of reporting increased sharply in 2004, mainly due to a major outbreak, but since then we have seen a steady decrease in reports, although it is now plateauing. We think this is mainly due to a reduction in the number of doctors / clinics at the Birmingham Chest Clinic.
The most common causes in 2011 were Isocyanates (15 cases), followed by Adhesives (7 cases).
Nearly all cases reported in 2011 were by the Birmingham Chest Clinic. We hope to increase the number notified by others this year by using the MTS website to contact notifiers. The most common method for the diagnosis of occupational asthma still remains a history of improvement of symptoms during holidays or periods off work.
The method of reporting to the Shield scheme has now changed and is done via the new version of the Oasys program that works through the internet. For those that use serial peak flows as a method of diagnosis this will greatly improve the ease of reporting. The data collected is all anonymous and so there are some changes in the data that we record, although it is largely similar.
Introduction
Shield is a joint project between the West Midlands branch of the Society of Occupational Medicine and the Midland Thoracic Society. The scheme, which was set up in January 1989, was established to meet three main objectives. 1) To study the general and specific incidence of occupational asthma within a defined geographic area, 2) To determine proposed mechanisms of asthma (we don't collect this anymore), and 3) to audit diagnostic methods and objectives.
The last report on Shield's progress was written for 2010 and summarised the information gained in that year, to that of previous years, 2009 and 2008. This report aims to update the participants of Shield by summarising the trends found in 2011 compared to those found in 2010 and 2009.
Outbreak of the year
The outbreak of latex asthma has been controlled by the replacement of latex examination gloves with vinyl/nitrile gloves and the use of powder free well washed latex gloves for surgical use. Despite this 2 workers with latex asthma were reported this year. One was a dental nurse in a small practice where the dentist was still wearing latex examination gloves, we have no information on the other.
Agent Awareness
Isocyanates have a habbit of appearing where you least expect them. A manufacturer of pre-fabricated dormer windows developed occupational asthma. The dormer windows had a wood frame, coated with fibreglass using a styrene-based resin (a rare cause of occupational asthma). He used an orbital sander with some local exhaust extraction, then applied a styrene-based bodyfiller and adhesive containing methyl methacrylate (a cause of occupational asthma) rubbing it down between coats. He used an epoxy sealant cured with phthalic anhydride (another cause of occupational asthma) before wiping the whole construction down with thinners and painting with a cellulose paint. Specific challenges with these agents were all negative. A workplace visit identified a booth where a polyurethane foam was sprayed onto the dormers for insulation, for customers who did not want the usual fibreglass insulation. The polyurethane was made by mixinging MDI (diphenylmethane di-isocyanate) with a polyol with little local exaust extraction. Although he didnt do this job, MDI challenge showed that his occupational asthma was caused by MDI. He has been relocated to a separate building manufacturing pre-fabricated porches using similar materials, but without insulation. Repeat Oasys records showed that he no longer had reactions related to work.
Shield Data
Number of Cases
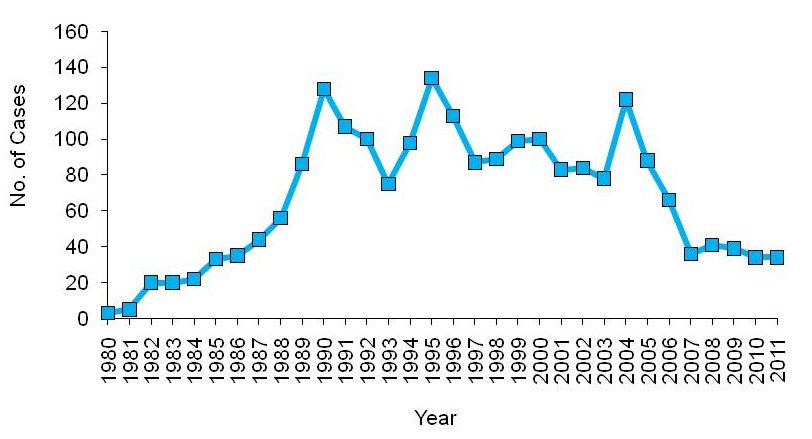
The number of cases of occupational asthma reported to the Shield scheme is 34 so far. It is difficult to compare notification for each year properly, as the last few years are likely to change, therefore the graph below is only as a guideline.
Figure 1 Number of cases diagnosed with occupational asthma between the years of 1980 and 2011
Personal details
In the year of 2011, 34 new cases have been reported to the scheme so far. As the data is anonymous we can no longer report the percentage of men and women. 28 (82%) of the new cases had no pre-existing asthma, 22 (65%) were non atopic and 18 (53%) had never smoked.
Reporting Hospital and Physician
The data is now collected anonymously so we are no longer recording the reporting hospital and physician.
Suspected agents at work
In 2011 the most commonly reported agent that workers were exposed to was Isocyanates (15 cases), followed by Adhesives. (7 cases). The 2 most common in 2010 were isocyanates and cleaning agents (13 and 9 cases respectively). Isocyanates were also the most common in 2009. 383 cases of isocyanate suspected asthma have now been reported to the scheme, the first case being in 1978. Metal working fluid exposed cases are decreasing with only 2 notifications being made in 2011.
The top reported agents in 2011 were as follows.
Employers and Jobs
The employer for a patient is encrypted when sent to the Oasys Internet Database for confidentiality reasons so it is no longer possible to report this. The jobs are still reported but we have found that job descriptions are very specific and there is rarely more than one patient for each type of job so we have stopped reporting these too.
Methods used for diagnosis
The methods used for diagnosis that are documented on the shield form are; 1) Improvement on holiday, 2) Improvement off work, 3) Serial peak flow charts, 4) Specific IgE, 5) Methacholine at work, 6) Methacholine away from work and 7) Specific bronchial provocation tests. 33 cases were documented as improving on holidays. There were 6 specific challenges performed on patients diagnosed in 2011.
| Method |
% 2011 |
% 2010 |
% 2009
|
| Improving on holidays |
97 |
91 |
85 |
| Improving off work |
88 |
88 |
82 |
| Serial peak flow |
91 |
82 |
82 |
| Specific IgE |
56 |
44 |
41 |
| Methacholine at work |
65 |
82 |
59
|
| Methacholine away from work |
38 |
35 |
18
|
| Specific Bronchial Challenges |
18 |
18 |
10
|
Proposed method of asthma
We no longer record the proposed mechanism of asthma.
Subsequent History
We no longer record the subsequent history.
Gold Standards
A gold standard occupational asthma case is defined by either; 1) Bronchial challenge test, 2) A four fold change in their bronchial reactivity with a good history, or 3) Positive IgE with a good history, and all of these can be accompanied by a good quality PEF record. 4 cases have become gold standards in 2011 so far. The database does not automatically record gold standard cases due to a fourfold change in bronchial reactivity any more, as there are a lot of different methods of measuring bronchial reactivity that all have different units.
BTS Audit Guidelines
The audit recommendations from the BTS Standards of care for occupational asthma (Fishwick D et al. Standards of care for occupational asthma, Thorax, 2008; 63 : 240-250) are now collected through Oasys. This is the second year that we have recorded adherence with the BTS Audit guidelines. The figures below show the percentage done by visit 2 or before. Specific IgE tests are not available for all agents, so this number is artificially low.
| |
% 2011 |
% 2010 |
% 2009 |
| Specific IgE |
56 |
44 |
|
| Occupational History |
94 |
79 |
|
| FEV1 / FVC |
97 |
85 |
|
| Serial Peak Flows |
91 |
82 |
|
| Employment Advice |
82 |
62 |
|
| Compensation Advice |
62 |
44 |
|
Future Developments
The new version of Oasys is working well and we are now using it to collect data. We are separating out the Shield data into this report. Data from all people using Oasys will now go into the Oasys Usage report, which will have global scope. We hope to colloborate with other surveillance schemes
Conclusions
Occupational asthma remains a serious disease causing much morbidity, and is potentially preventable. The Health and Safety Executive are currently emphasising the need to control occupational asthma.
.
Comments
Please sign in or register to add your thoughts.